Breast cancer is the most common cancer among women in the United States and the second leading cause of cancer death among women behind lung cancer. One in 8 women will develop breast cancer in their lifetime. Today there are over 2.6 million breast cancer survivors in the United States.


Public awareness of the disease and greater efforts for early detection with screening mammography have increased early detection of the disease, treatment and long-term survival. Early-stage localized breast disease is associated with a 98% 5-year survival rate. Treatment of breast cancer has evolved dramatically. Patients typically have an option for mastectomy or breast-conserving therapy (lumpectomy and radiation). In addition, a sentinel lymph node biopsy is performed to see if the cancer has spread beyond the breast. The final determination of your treatment plan will be determined by your surgical and medical oncologist. Your general surgeon may refer you to a plastic surgeon to discuss options for breast reconstruction. You also have the choice to discuss options for breast reconstruction regardless of the treatment plan. If you are a breast cancer survivor and now wish to have a reconstruction, you have the option to seek options for breast reconstruction after mastectomy.
Why Women Choose Breast Reconstruction
The diagnosis of any type of cancer can be overwhelming and scary. Patients often experience fear for their life and an urge to have the cancer removed immediately. Patients can be overwhelmed as they meet a team of doctors including medical oncologists, surgeons, and radiation oncologists. When confronted with information and decisions, patients may not feel ready to discuss breast reconstruction. One study showed only 40% of patients who have mastectomy go on to have breast reconstruction. The decision to have breast reconstruction is a personal one and there are multiple factors as to why women choose not to reconstruct their breast. Some women feel it is not a priority. Others don’t want to go through the additional surgery. Some women are afraid of the cost and think their insurance will not cover such a “cosmetic” procedure.
In 1998, Congress passed the Women’s Health and Cancer Rights Act which mandates that all insurance companies cover post-mastectomy reconstruction and symmetry operations to make both breasts look proportioned. Although the option for reconstruction is a personal one, the fact that more and more women choose to have reconstruction is a testament to the importance, safety and satisfaction of breast reconstruction. Ideally, the first stage of reconstruction can be performed at the time of the mastectomy to minimize the number of procedures and improve the cosmetic result. There are numerous studies validating the safety and patient satisfaction of breast reconstruction.

Patient Choices And Operative Technique: Implant Vs. Autologous
There are multiple options for breast reconstruction with evolving techniques that have improved the cosmetic outcomes. Reconstruction done at the time of the mastectomy is called “immediate” reconstruction whereas reconstruction done after mastectomy is called “delayed.” There are essentially two methods of reconstructing the breast: using breast implants (alloplastic) or using a patient’s own tissue (autologous). The breast reconstruction procedure of choice will depend on the patient’s preference, the stage of the breast cancer, and the patient’s anatomy. All things being equal, it will be up to the patient to decide if they wish to use an implant to reconstruct their breast or their own living tissue.

Types Of Reconstruction
Onco-Plastics
Implant
Onco-Plastics
Patients who are getting mastectomies are not the only ones who could benefit from a plastic surgeon. The term “Onco-Plastics” represents a growing new field highlighting the collaboration between the general surgeon and plastic surgeon in delivering the best oncologic and aesthetic surgical care for the patient. It is a principle that Dr. Jerome Liu and Dr. Tom Liu use for all their breast reconstruction patients. In patients with a large or hanging breast (also known as a “ptotic” breast), special incisions can be used to remove the tumor while reshaping and rejuvenating the breast. Working closely with your general surgeon or breast surgeon, Dr. Jerome Liu and Dr. Tom Liu will design skin excision patterns for ease of tumor access while maximizing healing and hiding the scar.
Implant
Implant reconstruction can be performed as a two-staged or one-stage operation. In the two-stage reconstruction, a tissue expander (temporary saline implant) is placed underneath the pectoralis major muscle (Stage 1). Additional coverage and support is provided by using a piece of acellular dermal matrix, one of the new cutting-edge techniques in breast reconstruction. Patients usually spend one day in the hospital overnight for pain control. During your follow-up, the plastic surgeon will begin expansion of the implant in the office until the final volume is reached. When the breast size is finalized, you will schedule the next stage of your reconstruction (Stage 2), which is typically 3 months after the first stage. The second stage is an outpatient procedure where the tissue expander will be removed and the final silicone implant will be placed. After the final size and shape of the implant is set, the reconstruction culminates with the reconstruction of the nipple followed by tattooing of the areola (office procedures). In certain unique cases, a tissue expander is not necessary and the final silicone implant is placed at the time of the first operation. Dr. Liu will help you determine which method is best for you.
Before & After





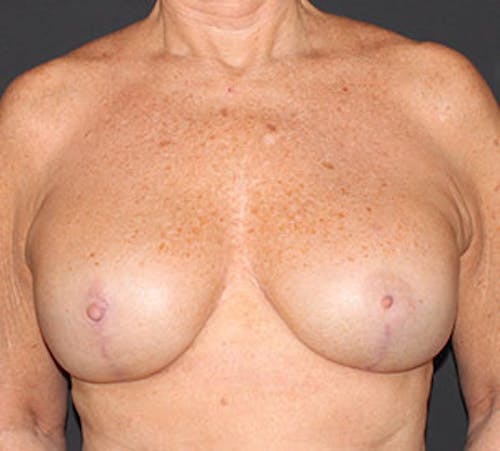




Warning:
This gallery contains nudity. Please click OK to confirm you are at least 18 years of age and are not offended by this material.
Ok
Summary
Breast reconstruction following mastectomy for the treatment of breast cancer is an option available to all women. Research publications continue to demonstrate that breast reconstruction is an integral part of breast cancer treatment with obvious psychological benefits without jeopardizing disease-free survival. Advances in breast reconstruction surgery continue to provide women with multiple surgical options, whether it is with newer generation silicone implants or the latest refinements in microsurgery-free flap breast reconstruction. The Women’s Health and Cancer Rights Act of 1998 mandates insurance coverage for not only the reconstruction but also the ensuing symmetry operations. Although the decision to reconstruct the breast is a personal one, we encourage you to seek a consultation with a plastic surgeon trained and dedicated to breast cancer reconstruction to discuss your surgical options along with your breast oncology surgeon.

Contact SVIA® Sacramento
Dr. Jerome Liu or Dr. Tom Liu are fellowship trained plastic surgeons and perform all aspects of breast reconstruction from implants to microvascular free flaps. SVIA® Sacramento is dedicated to advancing the reconstructive care of the breast cancer patient through research and community outreach. To discuss your options for breast reconstruction, please make an appointment with Dr. Jerome Liu or Dr. Tom Liu.

